
Partial Knee Replacement
If you have further questions about partial knee replacement then please feel free to contact us
here.
Alternatively you can book an appointment to see us below.




If you have further questions about partial knee replacement then please feel free to contact us
here.
Alternatively you can book an appointment to see us below.
Knee replacement surgery is reserved for end-stage arthritis when the articular cartilage (gristle) lining the bones has completely worn away. This arthritis may affect the whole knee or very commonly may only affect part of it. The knee has three compartments, the medial (or inner side) compartment, the lateral (outer side) compartment and the patellofemoral (kneecap) compartment. It is possible to perform a partial (or unicompartmental) knee replacement on each of these compartments separately.

Figure 1: X-ray of the left knee showing medial compartment arthritis
This is the most commonly affected compartment in the knee; one third of patients will have isolated medial compartment arthritis (see fig 1).
The symptoms are very similar to those patients who have arthritis throughout the rest of the knee joint. These are:
Patients with medial compartment arthritis commonly have a bow-leg deformity which they may have had for years. This often predisposes them to arthritis because the majority of the body weight passes through the inner side of the knee when weight bearing.

Figure 2: X-rays of the left knee following medial partial knee replacement
If the arthritis is severe (bone-on-bone) and function is severely compromised, then a knee replacement should be considered. This may be a partial (see fig 2) or a total knee replacement (TKR). In order to perform a partial knee replacement there are a number of criteria which need to be fulfilled. The joint deformity must not be too severe, there must be a near full range of motion and the knee ligaments must be intact.
The time taken to do the operation is very similar to TKR. However, the partial knee replacement is undertaken using minimally invasive techniques; this limits the degree of tissue damage which reduces postoperative pain and swelling. Infection rates are lower with partial knee replacement, range of motion has been shown to be greater and recovery time is quicker. The knee is also said to feel more like a normal knee in comparison to a TKR. The downside of the operation is that the rest of the knee may develop arthritis over time. This may require an operation to convert to a TKR, which is normally straightforward.
Isolated lateral compartment arthritis is seen more rarely (only 1 in 20 patients). Its symptoms are different to medial compartment arthritis. The pain is felt over the lateral (outer) side of the knee and there is a tendency to for the knee to give way; both of these may be made worse walking down stairs or an incline.
As with medial compartment arthritis, the options are a partial or total knee replacement. Lateral sided unicompartmental knee replacement is again performed using minimally invasive surgery and carries similar pros and cons to the medial replacement. As with the medial side there are two different designs of lateral replacement, fixed or mobile. The design is similar to the total knee replacement where the femur and tibia are resurfaced with a metal component while a tough plastic spacer (made of polyethylene) sits between. The subtle difference between fixed and mobile designs is that the plastic spacer in mobile designs is free to move as the knee bends and straightens, whereas in the fixed design the spacer is fixed to the top of the tibial component. Both function well, however many surgeons prefer a fixed type of design for the lateral side because there is a greater chance of the plastic spacer "popping out of joint" (dislocating).
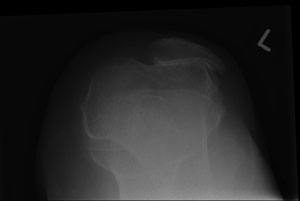
Figure 3: X-ray showing patellofemoral arthritis with bone-on-bone articulation
Isolated patellofemoral compartment (kneecap joint) arthritis (see fig 3) is seen in only 5-10% of patients. There may be a history of kneecap instability in the past which has led to wear and tear arthritis of the joint.
The most common symptom is pain which is classically felt over the front of the knee, but may also be experienced behind the knee. This pain is generally made worse going up and down stairs or an incline. Patients also struggle to sit for prolonged periods of time; driving may become difficult for this reason.
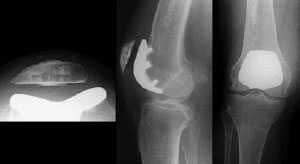
Figure 4: multiple X-rays of the knee following patellofemoral replacement
When the patients' symptoms fulfil the criteria for knee replacement surgery, the options are to proceed with patellofemoral replacement or TKR. Patellofemoral replacement (see fig 4) carries the same pros and cons that other types of partial knee replacement do. The final decision will need to be made by the patient.