
Posterior Cruciate Ligament (PCL)
If you have further questions or would like to discuss (PCL) injury and reconstruction then please feel free to contact us
here.
Alternatively you can book an appointment to see us below.




If you have further questions or would like to discuss (PCL) injury and reconstruction then please feel free to contact us
here.
Alternatively you can book an appointment to see us below.
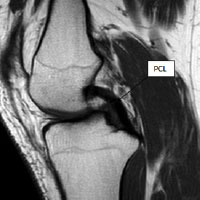
Figure 1: magnetic resonance imaging (MRI) scan showing native posterior cruciate ligament (PCL) connecting femur (thighbone) to tibia (shinbone)
The posterior cruciate ligament (PCL) is one of the less commonly injured knee ligaments. Like the anterior cruciate ligament (ACL) it connects the femur (thigh bone) to the tibia (shin bone) (see fig. 1). Its main role is to keep the knee stable during rapid acceleration and deceleration activities.
The PCL is most commonly injured when the front of the knee sustains a direct blow while the knee is bent. This classically occurs during road traffic accidents when the knee hits the dashboard, or when footballers and rugby players fall onto a bent knee. This forcefully pushes the tibia backwards at the knee rupturing the ligament. PCL tears may also occur when the knee is over flexed or extended and may be associated with other ligamentous injuries around the knee. These multi-ligamentous injuries are generally the result of high-energy trauma.
The knee may become very swollen after the injury (within a few hours) and it may be difficult to walk. The knee may feel unstable or give way and knee movement may be painful.

Figure 2: MRI scan showing complete tear of the posterior cruciate ligament
The diagnosis of PCL injury is usually made based on the description of the injury, your symptoms and a thorough visual and physical examination of the knee. The injured knee will be compared with the normal knee particularly assessing if there is any abnormal sag or movement of the tibia on the femur. An x-ray will be performed to exclude any bony injury and you will also require a MRI (see fig. 2) to assess the extent of the injury to other structures.
The initial treatment focuses on the acute injury. A useful acronym to remember is RICE, consisting of Rest, Ice, Compression and Elevation. Anti-inflammatory medication (e.g. ibuprofen) and painkillers (e.g. paracetamol) are of great importance in relieving swelling and pain.
Most patients with an isolated PCL injury can be managed without an operation (conservatively) and function well. In some patients, particularly those undertaking a very active lifestyle, the knee may just “not feel quite right” and may prevent them from performing at the level they would like. In addition, patients who have sustained injury to multiple ligaments including their PCL (combined PCL injuries) usually require early surgical repair.
The mainstay of conservative treatment is physiotherapy aimed at regaining full range of knee motion full muscle power and reducing swelling. Work is also required to develop the proprioceptive protective reflexes required to protect the joint during normal activities of daily living.
Research studies have shown that surgical reconstruction is best carried out on a pain-free, healthy joint with a full range of motion. Patients are referred to their physiotherapists who supervise their knee rehabilitation prior to reconstruction.
All surgical reconstructions of the PCL require a graft. Mr Barnett will either use sections of your own hamstring tendons (autograft) or use tissue from somebody else (allograft). The surgical technique uses rigid fixation of the graft with screws enabling rapid rehabilitation. Sometimes it is necessary to wear a brace to protect the knee.
Although PCL reconstruction surgery has a good chance of returning the knee joint to a good level of function and stability, the final result will depend upon the extent of the damage found within the knee joint; it will also depend on satisfactory rehabilitation having been undertaken.
You should inform your surgeon and anaesthetist of any medical conditions, previous operations or allergies as this may affect your operation. You must contact us before you go into hospital if there is any evidence of spots, ulcers or broken skin around the area to be operated on OR if you have a cold, cough or infection evident. If you are taking medication you must check with your surgeon and anaesthetist as to whether you need to stop taking any of the medication prior to your operation.
The most important factor determining success following surgery is postoperative rehabilitation. You will see the physiotherapist prior to discharge who will instruct you on exercises you should begin to work on. This is the start of a structured rehabilitation protocol supervised carefully by skilled physiotherapists. The graft is known to be weak in the first three months following surgery and it is our experience that rehabilitation should not be too aggressive.
These are rare complications, however, the combination of knee injury, immobilisation of the limb, smoking and the oral contraceptive pill or hormonal replacement therapy (HRT) all multiply to make the risk greater. You should inform Mr Barnett if you have any history of thrombosis. Smoking should be stopped a minimum of one week prior to surgery.
This is more common in patients taking aspirin or nonsteroidal anti-inflammatory drugs (NSAIDs) - such as naproxyn, voltarol and ibuprofen. These should be stopped at least one week prior to surgery. If there is a significant collection of blood within the knee, this may require draining.
It is common to notice bruising in the limb particularly in the thigh or around the wounds. Sometimes this may extend down to your ankle. Bruising is more common in patients taking aspirin or NSAIDs.
Surgery is undertaken in an operating theatre in an ultra-clean environment. In addition, antibiotics are used to reduce the risk of infection. Despite these measures, infection can still occur. This may present with a feeling of warmth and redness around the knee. It is imperative that you contact your surgeon prior to the commencement of any antibiotics.
It is very common to develop a patch of numbness close to your wounds. This is nothing to worry about and tends to shrink in size over time.
The hamstring muscles recover rapidly; tendon regrowth may be felt at two weeks following the operation. However, scar tissue which forms around the reforming tendons may tear. This may be felt as a pop or tear behind the knee. This problem usually occurs before the 6 week stage following surgery and may set your progress back a couple of days.
This is poorly understood and occurs in <1% of grafts.
Scar tissue build-up within the knee may limit range of motion following surgery. This requires intensive physiotherapy to correct.
A. General anaesthetic
A. Approximately 60-90 minutes.
A. Generally you will require only one night in hospital
A. Yes. You will need to walk with crutches for the first two weeks following surgery.
A. Physiotherapy is started immediately and is aimed at reducing swelling, regaining range of motion and muscle strength.
A. Yes, this is known as prehabilitation and is very beneficial.
A. Any blood thinning medication and hormonal preparations (such as the oral contraceptive pill) should be stopped. Your surgeon will inform you when the medication needs to be stopped.
A. Driving an automatic car is possible as soon as pain allows after left knee surgery. Should the right knee be involved driving is permitted when you are able to walk without crutches and can make an emergency stop. Always check with your insurance company before you drive.
A. After 2 months most of the swelling should have gone.
A. Sedentary and office workers may return to work approximately 1 week following surgery.
A. Return to competitive sport is permitted at 9-12 months following surgery, provided that there has been a complete rehabilitation
A. You will return for removal of the superficial dressings and a wound check at 2 weeks following surgery unless advised otherwise. Additional Links: AAOS website