
Collateral Ligament Injury
If you have further questions about collateral ligament injury then please feel free to contact us
here.
Alternatively you can book an appointment to see us below.




If you have further questions about collateral ligament injury then please feel free to contact us
here.
Alternatively you can book an appointment to see us below.
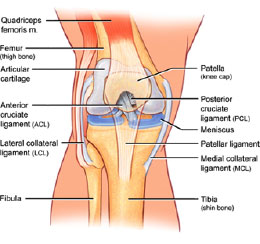
The collateral ligaments represent two of the four ligaments which hold the knee together. Unlike the cruciate ligaments which lie in the middle of the joint, the collateral ligaments are located on the inner and outer sides of the knee. The medial collateral ligament (MCL) connects the femur (thighbone) to the tibia (shinbone) and stabilises the inner (medial) side of the knee. The lateral collateral ligament (LCL) connects the femur to the fibula (the other bone in the lower leg) and stabilises the outer (lateral) side of the knee.
Medial collateral ligament (MCL) injuries are far more common than those to the LCL. They are commonly caused when the knee is bent inwards towards the other knee while the foot move outwards. This puts strain on the MCL and may either damage some of the fibres ("sprain") or completely tear the ligament. The injury causes sharp pain on the inner side of the knee.
The initial treatment focuses on the acute injury itself. A useful acronym to remember is RICE, consisting of Rest, Ice, Compression and Elevation. Anti-inflammatory medication (e.g. ibuprofen) and painkillers (e.g. paracetamol) are of great importance in relieving swelling and pain.
If the MCL is partially torn or "sprained", conservative treatment is normally all that is required. However, if the MCL is completely torn and the ligament fibres have no chance of joining up again, the MCL may need to be surgically repaired.
Regardless of whether the MCL injury is treated conservatively or surgically, you will need to wear a knee brace for approximately 6 weeks to help stabilise the knee and allow ligament healing to take place. During this time you will also need physiotherapy to help maintain range of knee motion and strengthen up the muscles at the front (quadriceps) and back (hamstrings) of the thigh.
After successful rehabilitation most patients return to their former level of activity.